eight.
Last Summer, we took Elliott to the beach for the first time. Technically, she had been to the beach before however, this time, she could splash in the water. This time, she could play in the sand. This time, I wasn’t worried about water and sand getting into her lungs via a hole in her neck. I was only worried about water and sand getting into her lungs via her mouth and nose. Ya know, like a regular parent.
I watched my daughter play with exuberance. She splashed incessantly; signing “water” over and over again in between splashes. Sitting in the surf in her bright pink rash guard, she beamed as the waves rushed around her. I’ve never known a child more deserving than my daughter of experiencing the way the ocean can make a person feel.

The path to the beach was not an easy one. In the March post I wrote about Elliott’s upcoming surgery. Below is something I wrote in the midst of walking that path; in the haunting, early morning hours of day eight.
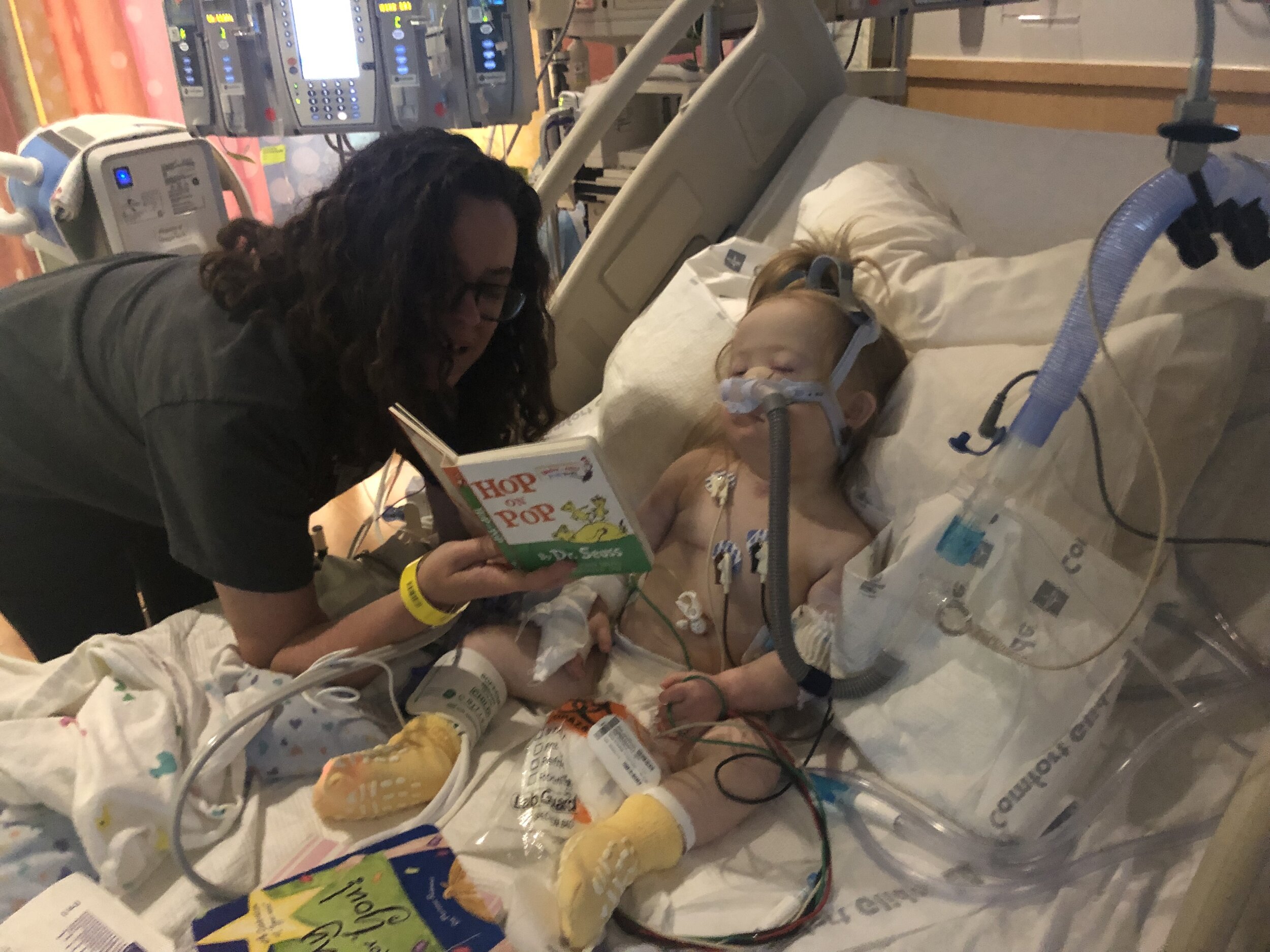
It’s 4 am. I’m sitting in a rocking chair in the PICU of Texas Children’s Hospital next to Elliott’s Bed. My eyes are dry. The kind of dry when you wake up in the middle of the night to use the bathroom - your bladder ready to awaken but not the rest of your body. Brad snores loudly in the corner trying to sneak in long overdue sleep on the fold out sofa bed. A baby cries in agony and confusion down the hall in another room. The machine ventilating my daughter offers soft and steady cadences of 12 breathes per minute.
Breath. .. Breath. .. Breath. .. Breath. ..
This Pediatric ICU is the Ritz-Carlton of ICU’s. We have our own room with a bathroom, rocking chair, mini desk, sofa that converts to a bed, TV with a significant variety of channels (not that we ever turned it on… not even once), ample space to move around, and a bathroom. Did I mention the bathroom? Our particular room has a wide sliding glass door with a curtain floating beside it; both to be closed anytime we desired a moment of privacy. A moment of fake escape from the world sitting just on the other side; awaiting our inevitable return.
I’m on day eight without my daughter.
Eight days without holding her, watching her scoot around on the floor, throw her toys, squawk adorably, or practice her sign language. Eight days without seeing her blue eyes or her chocolate pudding covered smile. Eight days of her being on such strong sedation and paralytic medication that she can no longer do any of the former. Rather, she is a tiny, 22 pound shell of herself laying in a hospital bed made for someone my size. I can’t help but wonder if she will be able to do all these things again.
Suddenly, as if he aims to free me from my own thoughts, I feel my son kick and adjust his position inside my belly. I am both tremendously grateful and overwhelmingly furious all at once. This complexity of emotions makes me cry as I sway in the rocking chair next to Elliott’s bed at 4 am. My eyes no longer dry.
Eight days before writing the above, Elliott had her trachea reconstructed. A major surgery, that went very well, followed by a long, winding and turbulent recovery full of uncertainty. She needed a posterior and an anterior graft in her airway, that translates to one on the front side and one on the back side. So her ENT surgeon removed a portion of her rib cartilage, cut it into two pieces and filed them down to the perfect measurements. The cartilage was sewn into two spots in her existing and flattened trachea; making it strong, open and round. A much better condition for breathing. The rib cartilage’s purpose for existence being changed forever.
If she had only needed the anterior graft, recovery time is 1-3 days. To add on a posterior graft, elongates that recovery to seven days.
Seven days on a ventilator that breathes for you via an intubation tube through the nose. Seven days not allowing movement. To move risks damaging the freshly reconstructed trachea before it’s healed and/or having the breathing tube come out before being ready to breathe without said tube. Both outcomes devastating therefore, sedation is required.
On day seven, the ENT medical team took our limp little girl to the operating room to remove the tube and give Elliott her first chance at breathing without a trach. I remember being skeptical of this plan from day one - paralyze someone for a week (voiding them of all existing energy resources and muscle strength) who has NEVER successfully breathed without medical devices, awaken them suddenly, and observe the confusion in their eyes as they struggle to inhale and exhale effective enough to stay alive. .. uhh.. what?
So yeah, it did not go well.
At first, upon immediate extubation, she was breathing independently. Appearing just strong enough so that her Doctor actually came back to the hospital room to inform Brad and I of Elliott’s success. Letting us know that she should be returning to our safe keeping very soon; breathing on her own…
I don’t remember how we reacted to this news once the Doctor left. Though after caring for Elliott for 2.5 years at that point, Brad and I have both developed a healthy (unhealthy?) skepticism of standard medical procedures. Our girl has never followed the typical path. Not even once. Therefore, I can confidently say we doubted that our girl would be coming back to us anytime soon, breathing on her own. (Though we certainly hoped we were wrong).
As predicted, after a long, worrisome time with no Elliott, we knew something wasn’t right. Her ENT Doctor returns to provide an update of what is happening in the OR. Turns out she was too heavily drugged to spontaneously breathe for more than a few minutes. Her body couldn’t keep up while also battling the paralytic and sedation medication still in her system. The team offered her multiple methods of assistance hoping she could overcome the drugs and breathe but alas… my baby could not.
She was re-intubated, re-drugged and re-turned to our hospital room as her medical team began to calculate a better approach for the next attempt.
Day one through six were hard.
Day seven was harder.
And we’d soon learn day eight through 24 would be hardest.
It was a balance. Elliott needed to be drugged enough to not pull the tube out of her nose but not too drugged to where she would again be unable to breathe unassisted. Knowing that the entire reason we were doing this surgery was to give our kid the chance to breathe, meant we needed to pull out all the stops to aid her. So, the drug drips were turned off, and we would try to extubate her again the very next morning. This meant that all night Brad, myself, and any brave medical staff we trusted were responsible for keeping her breathing tube in until 8 am the next day. A task that may seem simple, but for any of you that currently parent toddlers, have parented toddlers, or have been around toddlers… please tell me - How easy do you think it is to make them do… well, anything? Now imagine you have to make them keep a 10 inch tube stationary from the back of their throat, out through their nostril attached to a breathing machine so that they live. Yeah, this is a taaaad bigger than making her eat broccoli.
Stopping Elliott’s drugs was not the only change we were making in the game plan for this second extubation attempt - rather than taking her to the OR, it would be done in her hospital room with Brad and I present to assist. I was more than terrified to witness this event. Too close to home for when she failed extubation in the NICU and almost died. (12.1.2016 - this date tattooed on my psyche.) Despite the likely PTSD, I knew this was the right call - a child needs their parents. Especially a scared, disoriented child being asked to breathe in a new way. Her best chance at success was to be as drug free as possible and have her parents holding her, comforting her, encouraging her.
The closer we got to 8 am, the more wild Elliott became. Beginning at 6:30 am or so, one of her ICU Doctors, Dr. B., was holding her tube like he was holding onto the reigns of a bucking bronco at the rodeo. Elliott would make sudden thrashes of her head and Dr. B would calmly follow her with his whole body, never letting go of that tube. He stayed in the most uncomfortable position for 1.5 hours (never once complaining) until the ENT team arrived, finished setting everything up and exclaimed “Ok, it’s time”.
The plan:
Extubate Elliott.
Immediately put a mask over her nose hooked to a bi-pap machine giving her slight pressure support and oxygen because, well, why not.
Mom swoops in and picks her up..
..Oh God! Please give me tremendous strength in this moment. Let me comfort and calm her so she can have the best chance at breathing. I prayed for these abilities and shed a few tears, quickly wiping them away because Elliott did not need to see them. Her battle was much more immense than mine.
…
Ok, it was time. Brad and I stood towards the foot of Elliott’s bed, out of the way. There were roughly 7-10 medical folks in the room all having various roles to play.
Tube came out.
Bi-pap mask put on.
“Mom, you’re up” says Dr. M.
I conjure all the strength I can find, rush to Elliott’s bedside and scoop her up in my arms for the first time in eight days. I hold her head against my chest in my left arm, cradling her body in my right as she lay just on top of her brother, still in my belly. Blood from her mouth as a result of the extubation stains my blue, striped shirt. I hug her trembling little body (quaking uncontrollably from drug withdrawal), look deep into her hazy eyes and tell her that I know this is scary. I tell her I love her, that I am so proud of her and that it won’t always be this hard. Then, I immediately break into singing “The Wheels on the Bus”. She watched my mouth move, hushed her wimpers, and listened to the words of her favorite song as she breathed, calmly. Her body still trembling.
Brad and I take turns doing this for hours. (We sang that song likely a hundred times). Then, we progress from standing and rocking, to sitting and rocking, to finally snuggling her in bed.

I wore that blue-striped and blood-stained shirt for three days.
I can’t possibly recount the highs and very low, lows of days 8-24; so I won’t try. However, I can say that it was a couple weeks before we felt Elliott might actually depart the hospital with a scar of strength where a trach once was. Despite a very laborious journey, she did it. She learned to breathe unassisted and she learned to cough productively. After 24+ years of writing, I still can’t learn how to use their/there correctly without the help of Microsoft…meanwhile my child learns how to breeeeeathe in 24 days. She truly is extraordinary.

Overjoyed to be leaving the hospital… Elliott sporting her fresh scar of strength.
Confession: In total, I spent 7 hours shopping online for bathing suits for Ellie. Skimming store after store, finding the suits that were adorable and functional and perfect.
I bought three.
It seems absurd to have spent that much time and that much money on three swim suits that she likely won’t even fit into this Summer… but I don’t care. In the past, I refused to look at children’s bathing suits when shopping. I did look once, early on, and quickly learned how harsh and heavy the depression was that washed over me. I was a mother who was not able to give my child the experience of water - in any form. Lakes. Beaches. Pools. Splash pads. Full bath tubs. All basic requirements of childhood fun.
I didn’t think Elliott would be trach free until age 5 or 6. Maybe 4 if we were lucky. She did it in 2.5 years. One of her many moments proving me, and others, wrong. With all of my heart I hope she does not remember this hospital stay and what she endured. I hope she does not remember me faking strength as I held her weak body grasping for air on day eight. But I will. Forever.
I hope she only remembers the beach and the happiness she felt, because I will remember that too. Forever.
Until the NexT21,
Aubrey